
The first sign most people get that they have osteoporosis is a fracture. Not a fall, not a hard impact. Just a crack in a vertebra that happened because the bone was no longer strong enough to carry ordinary load. Patients describe it as a sudden sharp moment bending forward to pick something up, or a deep midline ache that started for no obvious reason and never fully went away.
We see this pattern in Lakewood Ranch: chronic lower back pain that never fully responds to care. A few weeks of rest, a round of anti-inflammatories, partial improvement. Then the pain returns, sometimes worse than before. The structural cause behind that pattern is different from disc herniation or facet dysfunction, and that difference matters because it changes what actually helps.
Osteoporosis affects an estimated 10 million Americans, with another 44 million in the osteopenia range where bone density is low enough to increase fracture risk. Most of those fractures are vertebral: the National Osteoporosis Foundation puts the annual vertebral compression fracture count at roughly 1.5 million. Most go undiagnosed for weeks or months because the pain can look almost identical to garden-variety mechanical back pain. Here is what is actually happening structurally, and what you can do about it.
What osteoporosis does to vertebral bone
Bone is not static. It breaks down and rebuilds constantly through a process called remodeling, driven by two cell types: osteoclasts (which resorb old bone) and osteoblasts (which build new bone). In young adults the cycle is roughly balanced. Around age 35, for most people, resorption begins to outpace formation. Bone mineral density (BMD) declines slowly and without symptoms for decades.
In osteoporosis, that imbalance is pronounced enough that structural integrity is genuinely compromised. The vertebral body, which is the roughly cylindrical weight-bearing portion of each vertebra, is composed largely of trabecular bone: a lattice-like internal scaffold that absorbs compressive load. Osteoporosis thins and gaps that lattice. The outward shape of the bone changes little; the internal structure becomes progressively less capable of absorbing normal daily forces.
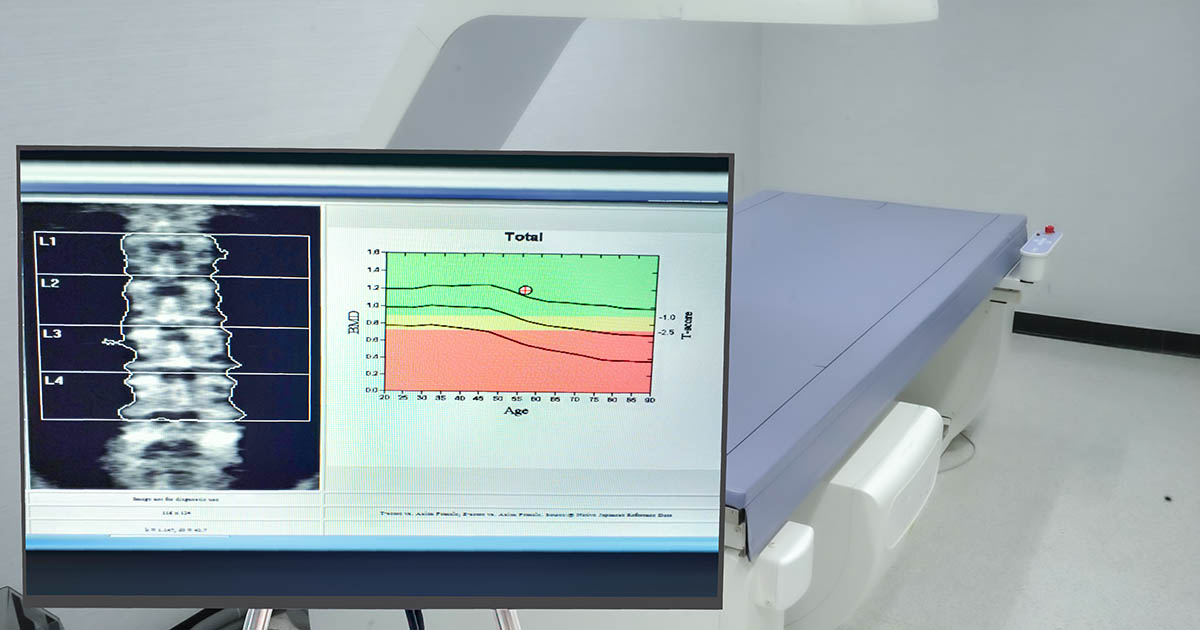
The DEXA scan (dual-energy X-ray absorptiometry) is the standard tool for measuring BMD. It produces a T-score comparing your bone density to that of a healthy 30-year-old. A T-score between -1.0 and -2.5 indicates osteopenia. A T-score below -2.5 is the clinical threshold for osteoporosis. Many patients arrive with a DEXA result on file from their primary care office but were never clearly told what it means for their spine specifically.
Three ways bone loss creates back pain
Vertebral compression fractures: The most direct mechanism. When trabecular bone is depleted enough, routine activity can generate enough compressive force to fracture one or more vertebral bodies. Bending forward to load the dishwasher, reaching overhead, a firm cough. The resulting fracture does not always produce dramatic acute pain. Some patients recall a specific sharp moment; others notice a gradual increase in midline thoracic or upper lumbar pain they attribute to muscle soreness.
Height loss and progressive kyphosis: Each compression fracture shortens the vertebral body slightly. Multiple fractures over time create measurable cumulative height loss, sometimes two or more inches across a decade. The resulting forward rounding of the thoracic spine (kyphosis) shifts load onto the lumbar segments below and accelerates degenerative disc disease at those levels. Patients often describe a change in posture they assumed was simply age.
Altered load distribution: Even before acute fracture, reduced vertebral stiffness changes how compressive force travels through the spine. The intervertebral discs, facet joints, and surrounding ligaments all respond to altered mechanics. This is one reason osteoporosis and disc degeneration frequently coexist in older patients, and why the same segment can show both problems on imaging at the same time.
Vertebral compression fractures: the most common osteoporotic injury
VCFs are estimated to affect roughly 25% of women over 50 and up to 40% of women over 80. Men are not immune: about one-third of all VCFs occur in men, typically 5-10 years later in the aging timeline than in women. The most commonly affected levels are T6 through L1, where compressive load is highest during routine activity.
The pain pattern is recognizable once you know what to look for:
- Midline thoracic or upper lumbar pain that began without obvious injury
- Worse with movement, position changes, and the sit-to-stand transition
- Often sharpest in the morning during the first few minutes upright
- Point tenderness directly over one or two spinous processes
- Sometimes accompanied by a mild sensation of giving way during activity
- Partial relief with lying down and full supported back rest
Most VCFs are managed conservatively. Many heal with 8-12 weeks of modified activity, appropriate bracing, pain management, and pharmaceutical bone-building support coordinated with the patient's physician. The chiropractic question is what the surrounding soft tissue, adjacent discs, and stabilizing muscles need during and after that process, and whether conditions like spinal stenosis have developed at the involved levels.
Who is at highest risk in Lakewood Ranch and the surrounding area
Certain factors accelerate bone loss well beyond the baseline age-related decline. The patient population in Lakewood Ranch, Bradenton, and Sarasota skews heavily toward the age bracket where these factors matter most.
- Post-menopausal status (estrogen loss significantly accelerates osteoclast activity)
- Long-term corticosteroid use (prednisone and similar drugs directly suppress osteoblasts)
- Low calcium and vitamin D intake sustained over decades
- Sedentary lifestyle (bone density responds to mechanical load: less movement means less rebuilding stimulus)
- History of smoking or heavy alcohol use
- Small frame and low body weight
- Family history of osteoporosis or fragility fractures
- Prior fracture from minimal trauma after age 50
Patients on long-term proton pump inhibitors (PPIs for acid reflux) are also at elevated risk. PPIs reduce calcium absorption by lowering stomach acidity, a fact that is often not clearly explained at the time of prescribing. If you take a PPI daily and have not had a DEXA in the past two years, that conversation is worth having with your primary care provider.
A spine that looks normal on a standard X-ray can be severely osteoporotic. The lattice structure of trabecular bone does not show reliably on plain films until density is already quite low. DEXA is the appropriate screening tool, and most insurance covers it for women over 65 and for men and younger women with risk factors.
Warning signs that back pain may be bone-related
Most back pain we evaluate is mechanical: disc herniation, facet joint dysfunction, sacroiliac instability, muscle guarding. Bone-related pain has a somewhat different clinical signature. These patterns are worth raising with your provider:
- New midline thoracic or upper lumbar pain without a clear triggering injury
- Acute sharp pain that followed a minor activity (coughing, sneezing, bending forward)
- Progressive height loss over several years
- Worsening thoracic kyphosis (a noticeable forward rounding that was not there a few years ago)
- Back pain that produces point tenderness directly over one or two vertebrae
- Chronic back pain that has not responded to standard conservative care despite reasonable effort
A separate category warrants prompt physician evaluation rather than a chiropractic intake: back pain accompanied by fever, significant night sweats, unintentional weight loss, or radiating pain into both legs simultaneously. These patterns require imaging and workup to rule out infection, malignancy, or significant cord involvement before any conservative care begins.
What conservative care can do (and the important caveats)
Chiropractic care for patients with known or suspected osteoporosis looks different from standard high-velocity manipulation. Thrust techniques directed at structurally compromised vertebrae carry real risk. Correct evaluation changes the approach, and the approach can still accomplish quite a bit.
The tools that are both safe and genuinely useful in bone-compromised spines include:
- Low-force mobilization and soft-tissue work to address surrounding muscle guarding and compensation patterns that develop around a painful or fractured segment
- Postural retraining to reduce the forward load on vulnerable thoracic vertebrae over the course of a normal day
- Spinal decompression, which creates negative intradiscal pressure without the compressive and rotational forces involved in manipulation. For patients with concurrent disc involvement and stable (not acutely fractured) osteoporotic vertebrae, decompression can be a useful component of the plan
- Core stabilization work to reduce reliance on passive spinal structures
- Movement education: how to lift, how to rise from a chair, how to transition from floor to standing in ways that reduce fracture risk
For patients who have developed spinal stenosis secondary to kyphotic deformity or compressed vertebral bodies, flexion-distraction and specific positioning protocols can also be appropriate in the right clinical context. The conversation about pharmaceutical bone-building therapy (bisphosphonates, teriparatide, denosumab) goes to the patient's physician or endocrinologist: those medications are outside chiropractic scope but are a significant part of the overall picture, and coordinating care between providers is standard here.
What the evaluation process looks like at our Lakewood Ranch clinic
Most patients referred or self-referred for osteoporosis-related back pain arrive with a DEXA on file, or need guidance on getting one. The clinical exam focuses on four things: range of motion and postural assessment; palpation of the thoracic and lumbar spine for point tenderness (a finding that suggests active or recent fracture rather than healed bone); neurological screening to identify any cord or nerve root involvement; and review of available imaging.
In 23 years of practice, Dr. Banman has seen many patients with chronic back pain that turned out to have a bone density component that prior treating providers had not identified or had not accounted for in the treatment approach. That is not a criticism: the pain pattern can be deceptive, and osteoporosis is often asymptomatic until something fractures. The practical point is that knowing the underlying diagnosis changes what is safe to do, what the realistic timeline is, and which additional providers need to be in the loop.
If your back pain has not responded the way you expected, bone density is worth adding to the list of things that have been checked.


