Herniated disc, you don't have to have surgery.
A herniated disc is when the soft inner core of a spinal disc pushes through a tear in its outer ring and presses on a nearby nerve. The pain can be sharp, electric, and frightening, but research shows the vast majority of herniated discs heal without surgery when conservative care is done well.
- Non-surgicaldecompression-first care
- 6-12 weekstypical improvement window
- 23+ yrsDr. Banman's experience

From healthy to herniated, the anatomy.
A herniated disc is easier to understand from above. This cross-section of a lumbar vertebra shows the soft jelly core, the tough outer ring that holds it in, the canal carrying the nerve bundle, and the nerve root exiting to the leg. Tap a marker to see what each part does and how a herniation happens.
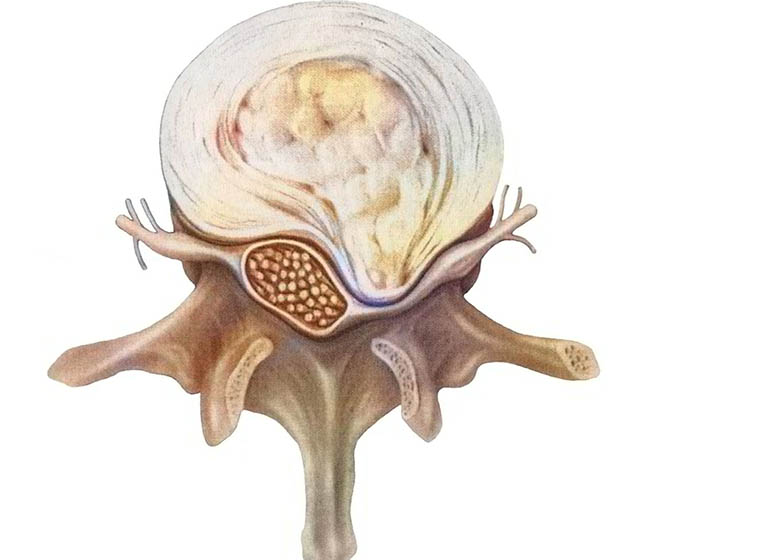
The nucleus (jelly center)Each disc has a soft gel core. When the tough outer ring tears, this jelly pushes out, that is a herniation. The escaped material can press a nerve and send pain, numbness, or weakness down the leg.
The annulus (outer ring)Concentric bands of fibrous cartilage normally lock the nucleus in place. Age, repeated strain, or one bad load can crack these rings and let the core escape.
The spinal canalThe nerve bundle runs through this central tunnel. A disc that bulges backward narrows the canal and crowds the nerves inside it.
The exiting nerve rootA nerve leaves the spine on each side at every level. A herniation aimed at that exit pinches a single root, producing the classic one-leg band of sciatica.
Tap a marker to explore
Why discs herniate.
Herniations almost never happen from a single moment, even when one moment is what you remember. The disc was usually already weakening.
Years of compression
Sitting, bending, lifting, repetitive flexion. Over time the outer ring of the disc accumulates microscopic tears that finally give way.
Sudden lifting injury
The "I bent over to pick up the laundry" moment. Real, but usually the final straw, not the only cause.
Disc degeneration with age
Discs lose water content as we age. A dehydrated disc has a stiffer, more fragile outer ring and is more likely to crack.
Genetic predisposition
Some families have weaker disc collagen, herniations show up earlier and at multiple levels.
Trauma or whiplash
A car accident, fall, or sports impact can herniate a previously healthy disc. Cervical discs are common after rear-end collisions.
Heavy work or sport
Construction, nursing, manufacturing, powerlifting. Jobs and sports that load the spine in flexion are the most disc-hostile.
Decompression-first, layered care.
The plan is built around the disc itself. Take pressure off it, calm the inflamed nerve root, restore motion to the surrounding joints, and rebuild the support around it.
Spinal Decompression
Gentle, targeted traction that may help create negative pressure inside the disc, encouraging the herniated material to retract.
Learn more →Chiropractic Adjustments
Restores motion to the joints above and below the herniated level, so the disc isn't taking all the load.
Learn more →Class IV Laser
Targets inflammation around the irritated nerve root and the surrounding soft tissue.
Learn more →EMS & rehab
Activates the spinal stabilizers that protect the disc through daily life, so improvement holds.
Learn more →Bulge, herniation, sequestration: what's the difference?
These words get used interchangeably but they describe distinct stages of the same problem. Knowing where you are on the spectrum helps clarify what to expect.
Disc bulge (also called protrusion)
The disc pushes outward symmetrically or asymmetrically but the outer ring (the annulus fibrosus) is still intact. The nucleus is contained, just displaced. Many bulges are completely silent and only show up incidentally on imaging. When a bulge causes symptoms, it is usually because it is bulging directly into a nerve root or the spinal canal. Conservative care, including spinal decompression and chiropractic adjustments, often handles bulges well.
Herniation (also called extrusion)
The outer ring tears and the inner nucleus material pushes through that tear. The herniated fragment usually stays attached to the parent disc but now sits where the nerve root runs, and the inflammatory chemistry of the nucleus itself can irritate the nerve even more than the physical pressure does. This is the classic "slipped disc," and despite the dramatic name, research suggests the body can shrink and reabsorb herniated fragments over time in most cases.
Sequestration
A piece of the nucleus breaks completely free from the parent disc and floats in the canal as a free fragment. Sequestered fragments paradoxically sometimes resolve faster than contained herniations because the body's immune system can attack and clear free material. Most sequestrations still respond to conservative care, though surgical consultation is more common at this stage if there is progressive weakness or loss of bowel/bladder control.
Quick answers.
Can a herniated disc heal without surgery?
Yes. Research consistently shows that most herniated discs improve substantially with non-surgical care over a period of weeks to months. The herniated material can shrink, retract, or be reabsorbed by the body. Spinal decompression, adjustments, and time are the conservative cornerstones. Surgery is reserved for cases with progressive neurologic deficit, severe weakness, or cauda equina syndrome.
How long does a herniated disc take to heal?
Most cases improve meaningfully in 6 to 12 weeks of consistent conservative care. Pain often eases first, followed by numbness, then weakness, which can take longer to fully recover. Severe or chronic cases sometimes need 4 to 6 months of care to feel resolved, and the underlying disc continues to remodel for up to a year.
Is walking good for a herniated disc?
Gentle walking is usually one of the best early activities. It keeps the spine moving, encourages disc nutrition through the pumping action of motion, and avoids the deconditioning that bed rest causes. If walking sharply increases the leg pain, that is a signal to ease back and have the case re-evaluated.
What movements should I avoid?
In the acute phase, avoid heavy lifting from a bent-forward position, repeated bending and twisting at the waist, and long stretches of seated flexion (couch, car, desk slouch). These positions load the back of the disc, exactly where the herniation usually sits. Specific guidance changes as you heal, we update it visit by visit.
Do I need an MRI for a herniated disc?
Not always. Dr. Banman's exam can usually identify a disc-related pattern from history, orthopedic tests, and neurological signs. We order an MRI when the findings would change the plan, when red flag symptoms are present, or when conservative care has not produced expected change in a reasonable window. Imaging without a clinical reason is not always helpful: many people have herniations on MRI with no symptoms at all.
Will I be in pain forever?
For the majority of patients, no. The disc itself can heal, and even when imaging shows residual herniation, the symptoms can fully resolve. Long-term outcome studies on conservative herniated disc care are encouraging: most patients return to normal activity and stay there.
Is decompression safe with a herniation?
Yes, when applied by a trained provider after a thorough exam. Decompression is non-surgical, non-invasive, and uses gentle, targeted traction to reduce intra-discal pressure. It is contraindicated in a small set of cases (recent fusion, severe osteoporosis, certain tumors, active infection), and that is exactly what the initial consultation rules in or out.
Insurance?
Chiropractic adjustments may be covered. Spinal decompression is typically not covered by insurance. HSA/FSA accepted. Payment options →
When to come in sooner.
Most herniated discs are an urgent problem, not an emergency. But a small subset of symptoms means same-day evaluation.
Loss of bowel or bladder control
This is the one true emergency, a sign of cauda equina compression. Go to the emergency room first, then call us.
Progressive weakness
If you can feel a leg or arm getting weaker over days, not stronger, that is a signal to be evaluated quickly. Earlier intervention preserves function.
Saddle numbness
Numbness in the area that touches a bicycle seat is another cauda equina warning sign. Emergency department first.
Pain not improving after 2+ weeks
Sharp back pain or sciatica that has not changed at all in two weeks is a sign the body needs help. A structured plan usually moves the needle.
Fever or unexplained weight loss with back pain
Uncommon, but it changes the workup. We coordinate with your primary care if that picture is present.
History of cancer
New back pain in someone with a cancer history warrants imaging before a treatment plan. We do not skip that step.
Most discs heal. Let's see what yours needs.
An honest exam, an honest plan. Quickest path is a phone call.