Vertigo, the spinning has a real source.
That sudden room-spinning when you roll over in bed, or the off-balance fog that won't quit? Vertigo and dizziness are not vague problems, they have specific, identifiable causes. We screen for each one (BPPV, upper cervical, vestibular) and either treat it or refer you to who should.
- BPPV-trainedEpley maneuver in-office
- Upper cervicalscreening & care
- 23+ yrsDr. Banman's experience

Inner ear, upper neck, or both.
The balance system lives in three fluid-filled semicircular canals in the inner ear. Tiny calcium crystals (otoconia) normally sit anchored in the utricle. When they break loose and float into a canal, the brain gets the wrong motion signal. The upper cervical spine feeds in too, which is why neck dysfunction can mimic inner-ear vertigo.
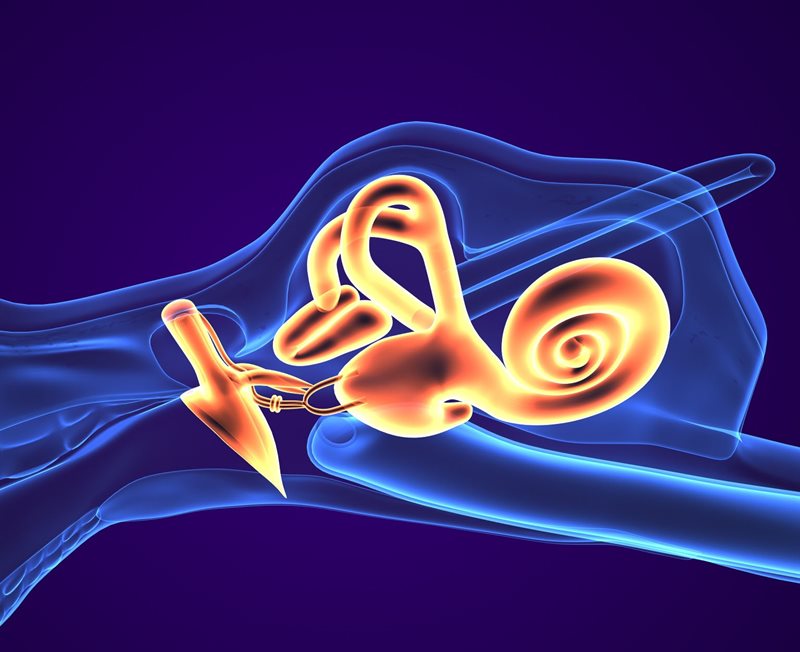
Semicircular canalsYour motion sensors, filled with fluid. In BPPV, loose calcium crystals drift into a canal and fire false spinning signals when you roll over or look up.
Utricle and crystalsWhere the balance crystals normally sit anchored. When they break free, the room spins. A gentle repositioning maneuver guides them back, and we check the upper neck too.
Tap a marker to explore
- BPPV (most common)crystals in a canal, brief intense spins triggered by head position
- Cervicogenic dizzinessupper-neck dysfunction confusing the balance system, often paired with neck pain
- Vestibular neuritisinner-ear nerve inflammation, often after a virus, constant spinning for days
- Meniere's diseaseepisodes of vertigo plus ringing in the ear and hearing changes
What's actually making the room spin.
Vertigo isn't a diagnosis, it's a symptom. The job of the first visit is figuring out which of these is the actual driver.
BPPV (the most common)
Calcium crystals dislodged from the utricle, floating in a semicircular canal. Brief intense spinning triggered by rolling over, looking up, or lying down. The Epley maneuver usually resolves it.
Cervicogenic dizziness
Dysfunction of the upper cervical spine (C0-C1-C2) sending faulty signals to the balance system. Usually paired with neck pain or stiffness and often follows a whiplash injury.
Vestibular neuritis
Inflammation of the inner-ear balance nerve, often after a viral illness. Sudden severe spinning lasting days, then gradually settling. Conservative care while it heals.
Meniere's disease
Episodes of severe vertigo plus tinnitus and fluctuating hearing in one ear. Requires ENT specialist care, we refer.
Migraine-associated vertigo
Vestibular migraine produces dizziness with or without headache. Triggers and treatment differ from inner-ear causes.
Cardiovascular & medication causes
Blood-pressure drops, dehydration, certain medications, and sometimes more serious vascular issues. Part of the screen.
Specific to the cause, never a guess.
There is no one-size-fits-all vertigo treatment. The first job is finding the cause; the second is the right targeted intervention.
Epley Maneuver (for BPPV)
A specific sequence of head and body positions that physically moves the displaced crystals out of the canal and back into the utricle. Often one-and-done.
Learn more →Upper Cervical Care
Targeted adjustments at C0-C1-C2 for cervicogenic dizziness. Often paired with soft-tissue work and posture correction.
Learn more →Class IV Laser
For inflamed upper-cervical soft tissue or neck-related contributors to dizziness.
Learn more →Vestibular Rehab Referral
For cases that need it, we refer to vestibular physical therapy. We don't pretend to do what we don't do.
Learn more →Vertigo, dizziness, lightheadedness, are they the same?
They get used interchangeably but mean different things, and the difference points to the cause.
True vertigo, the room spins
An illusion of motion. The world appears to spin, tilt, or move around you, or you feel yourself spinning even though you are still. True vertigo almost always points to either the inner ear (BPPV, vestibular neuritis, Meniere's) or the central balance system (brainstem, cerebellum). The duration matters: seconds-to-a-minute episodes triggered by head movement suggest BPPV. Constant spinning for days suggests vestibular neuritis. Recurring episodes with ringing in the ear suggest Meniere's. Our first task is sorting the pattern.
Disequilibrium, off-balance without spinning
Feeling unsteady on your feet without a true spinning illusion. Common with cervicogenic dizziness, bilateral inner-ear weakness, age-related multifactorial imbalance, or neurological conditions. This is where upper cervical care often shines: restoring proper motion at C0-C1-C2 can reduce the faulty proprioceptive input that confuses the balance system. We screen the neck carefully on every dizziness consultation, because neck involvement is missed embarrassingly often.
Lightheadedness, faint-feeling
A pre-faint sensation, like you might pass out. This is usually a cardiovascular signal, not an inner-ear one. Common causes include orthostatic hypotension (blood pressure dropping on standing), dehydration, medication side effects, anemia, or arrhythmias. Lightheadedness should be evaluated by your primary care physician or a cardiologist, not treated as vertigo. The differentiating question at our first visit is always: does the room actually spin, or do you just feel faint? Those are different problems.
Quick answers.
Can a chiropractor help with vertigo?
Sometimes, yes. The role depends on the cause. For BPPV (displaced inner-ear crystals), a trained chiropractor can perform the Epley repositioning maneuver. For cervicogenic dizziness driven by upper cervical dysfunction, targeted adjustments can be highly effective. For true inner-ear disorders like Meniere's or vestibular neuritis, chiropractic is not the primary treatment, and we refer to ENT or vestibular rehab as appropriate.
What is the most common cause of vertigo?
BPPV (benign paroxysmal positional vertigo) is by far the most common cause overall. It happens when small calcium crystals in the inner ear become dislodged and float into one of the semicircular canals, where they confuse the balance system. The classic giveaway is brief intense spinning triggered by rolling over in bed, looking up, or lying down. A single Epley maneuver resolves most BPPV cases within 24 to 48 hours.
How long does vertigo last?
BPPV episodes typically last seconds to under a minute per trigger but can recur many times a day until treated. A single Epley maneuver resolves most BPPV cases within 24 to 48 hours. Cervicogenic dizziness usually improves over a course of care of several visits. Vestibular neuritis can take weeks to fully settle even when handled correctly.
Is vertigo dangerous?
Most vertigo is not dangerous in itself, but the falls it can cause are. Sudden new vertigo with neurologic warning signs (severe headache, slurred speech, weakness, numbness, double vision, trouble walking) is a medical emergency, not a chiropractic visit, and should go to the emergency room immediately to rule out a stroke. We screen for these red flags on every dizziness consultation.
Why does my vertigo flare when I roll over in bed?
That is classic BPPV. Rolling over in bed changes the orientation of the displaced crystals within the canal. Their movement deflects the canal's sensory hairs and tells your brain the head is rotating rapidly, even though it isn't. The brain mismatches that signal against vision and proprioception, and the result is the spinning sensation. The Epley maneuver moves the crystals out of the canal so this stops happening.
Can neck problems really cause dizziness?
Yes. The upper cervical spine has rich proprioceptive input feeding into the same balance integration centers that handle inner-ear signals. When C0-C1-C2 are dysfunctional, often after whiplash or sustained poor posture, that input becomes noisy and the brain has trouble reconciling it with what the inner ear and eyes are reporting. The result is dizziness, disequilibrium, sometimes nausea, often paired with neck pain or headaches.
Can vertigo come back after the Epley?
BPPV does have a recurrence rate, somewhere around 15 to 50 percent over a few years, depending on the study. The good news is that the Epley works just as well the second or third time as it did the first. Some patients learn a home version (the Epley or the Brandt-Daroff exercises) for self-management when they feel an episode starting.
Insurance?
Chiropractic care including the Epley maneuver may be covered. HSA/FSA accepted. Payment options →
When dizziness is a 911 call.
Some dizziness presentations need an emergency department, not a chiropractor. We want you to know the difference.
Severe sudden headache with dizziness
A "worst headache of my life" combined with new dizziness is a vascular emergency until proven otherwise. ER first.
Slurred speech, facial droop, or arm weakness
Classic stroke signs. Call 911 immediately, do not wait, do not drive.
Double vision or vision loss with dizziness
Suggests central nervous system involvement. Emergency evaluation.
Numbness or tingling on one side of the body
Another stroke red flag with vertigo. ER.
Loss of consciousness or near-faint
That points to a cardiovascular cause, not an inner-ear or neck cause. Needs a primary care or cardiology workup before chiropractic care.
Sudden hearing loss with vertigo
Could be Meniere's, labyrinthitis, or rarely a vascular event. Same-day ENT or ER, not us first.
Let's find yours.
An honest screen, an honest plan. We refer when we should. Quickest path is a phone call.