Piriformis syndrome, the sciatica that isn't from your disc.
Deep, achy buttock pain that gets worse after a long drive or a day at the desk, sometimes shooting partway down the leg? That's often the piriformis, a small muscle deep in the glute, irritating the sciatic nerve as it passes underneath. Different cause, different treatment, real relief.
- Non-surgicalconservative-first care
- Shockwave + softwavefor stubborn trigger points
- 23+ yrsDr. Banman's experience

Why your sciatica may not be from your disc.
The piriformis runs from the sacrum to the top of the femur, and the sciatic nerve passes right underneath it (and in about 15% of people, straight through it). When the piriformis tightens or spasms, it presses on the nerve and mimics a disc-driven sciatica almost perfectly.
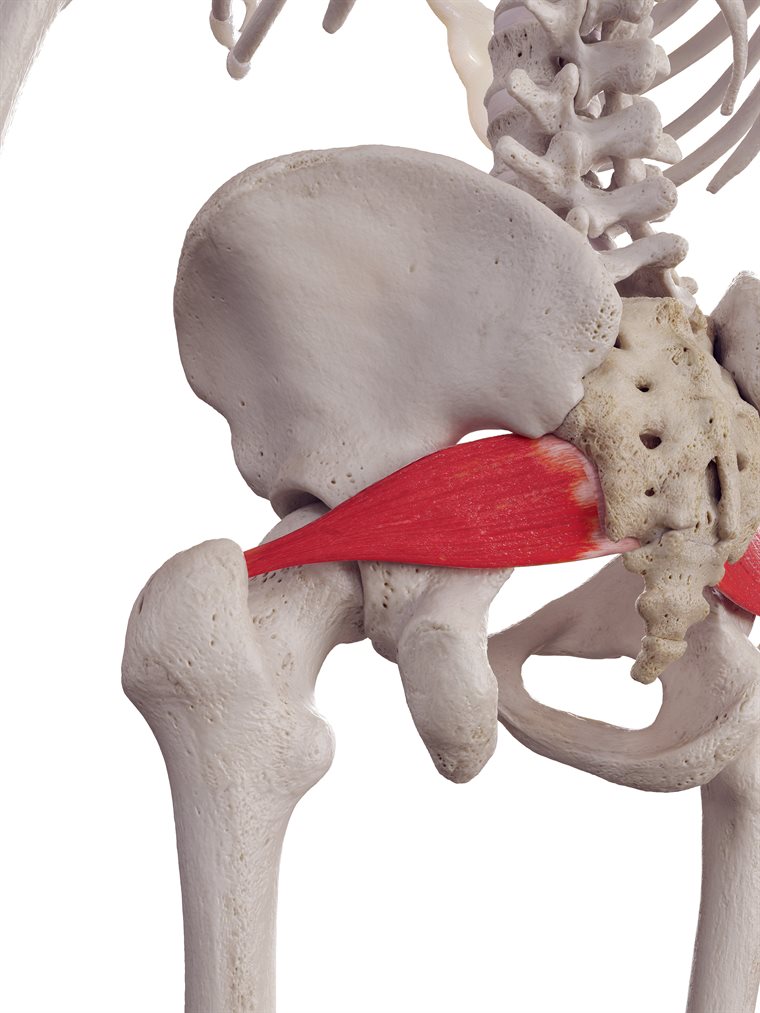
PiriformisA small, deep buttock muscle running from the sacrum to the femur. It tightens with prolonged sitting, driving, or a back-pocket wallet.
Where it pinchesThe sciatic nerve passes right under the piriformis, through it in about 15% of people. A tight muscle squeezes the nerve and produces sciatica that is not from a disc.
Tap a marker to explore
- Where it hurtsdeep mid-buttock, sometimes radiating down the back of the thigh
- What makes it worseprolonged sitting, driving, climbing stairs, wallet in the back pocket
- What helpsstanding up to walk it out, lying flat, gentle stretching
- How we treat itshockwave/softwave for the trigger points, manual therapy, graded stretching
Why the piriformis gets cranky.
The piriformis is small, deep, and easy to overload. A few patterns produce the vast majority of cases.
Prolonged sitting
Desk jobs, long drives, cycling. Hours of compression on the muscle and the underlying nerve. Easily the most common contributor.
Wallet in the back pocket
Yes, really. A thick wallet over the piriformis, day after day, can produce the entire syndrome. Called "wallet sciatica" for a reason.
Sudden increase in running or hill work
The piriformis stabilizes the hip during single-leg loading. Ramp up too fast and it overloads.
Hip mechanics problems
Stiff hip flexors, weak glute meds, dysfunctional SI joints, all force the piriformis to do work it was not built for.
Direct trauma
A fall onto the buttock, a hard tackle, a kick. Sometimes the inciting event is obvious, more often the trauma fades and the piriformis stays angry.
After spine surgery or chronic back pain
When the lumbar spine has been protective for a long time, the piriformis often takes on stabilizing work it cannot sustain.
Release the muscle, calm the nerve, fix the upstream.
The trick with piriformis is not just stretching it harder. It is identifying what is making it angry, and treating both the muscle and the upstream contributors.
Shockwave Therapy
Acoustic waves disrupt chronic trigger points in the piriformis and break the cycle of spasm. Particularly useful for stubborn cases.
Learn more →Softwave Therapy
Drives a regenerative response in the muscle and surrounding tissue. Pairs well with shockwave for chronic piriformis.
Learn more →Adjustments & manual therapy
SI joint and lumbar adjustments reduce the upstream demands on the piriformis. Direct soft-tissue release of the muscle itself when tolerable.
Learn more →Class IV Laser
Calms the inflammation in the surrounding tissue and the irritated sciatic nerve fibers.
Learn more →How we separate piriformis from a disc problem.
Sciatica is a symptom pattern, not a diagnosis. Differentiating the cause is the difference between treatment that works and treatment that does not.
The classic disc pattern
Disc-driven sciatica typically gets worse with forward bending, prolonged sitting in flexion, sneezing, coughing, or straining on the toilet. Pain often shoots beyond the knee and may include foot numbness or weakness lifting the big toe. Straight-leg raise reproduces it. The pain usually starts in the lower back and travels into the leg. An MRI, when needed, often shows a corresponding disc bulge or herniation. Decompression and adjustments handle most of these well.
The classic piriformis pattern
Piriformis-driven sciatica is centered in the deep buttock, not the back. It is reproduced by direct pressure on the mid-buttock, by sitting on a hard chair for 15+ minutes, by climbing stairs, or by certain stretches of the hip. Pain usually stops at the knee or only barely makes it into the upper calf. There is rarely true motor weakness or distal foot numbness. The straight-leg raise is often negative; the FAIR test (flexion, adduction, internal rotation) is often positive. Imaging is usually normal. Treatment focuses on the muscle and the upstream hip mechanics.
Why this matters for your treatment plan
If we treat a disc problem as if it were piriformis (stretching, trigger point work, no decompression) you will not improve, and may get worse from the stretching. If we treat a piriformis problem as if it were a disc (decompression for weeks without addressing the muscle) you will not improve either. The exam on Day 1 differentiates them with high accuracy, and the plan flows from that. About 6% of all sciatica cases are pure piriformis; another 10-15% have a piriformis contribution layered on top of a disc problem.
Quick answers.
How is piriformis syndrome different from sciatica?
Sciatica is a symptom (nerve pain down the leg), not a diagnosis. The most common cause is a disc problem in the lower back; piriformis syndrome is the second most common. Disc-driven sciatica is usually worse with bending, sitting in flexion, sneezing, or coughing. Piriformis-driven sciatica is usually worse with prolonged sitting (especially on a wallet), driving, or pressing on the mid-buttock. The exam differentiates them, and the treatment is different for each.
How long does piriformis syndrome take to heal?
Most cases improve substantially within 4 to 8 weeks of consistent conservative care. Stubborn chronic cases sometimes need 12 weeks or longer. Shockwave and softwave therapy can shorten the recovery curve in cases that have not responded to stretching and manual therapy alone.
Should I stretch the piriformis?
Usually yes, but the right way. Aggressive over-stretching of an already-irritated piriformis can worsen the symptoms. We teach a graded stretching protocol along with hip-mobility work that addresses the upstream contributors, not just the muscle itself.
Does sitting make piriformis syndrome worse?
Yes, prolonged sitting is one of the most consistent aggravators. The piriformis sits directly under the sciatic nerve and gets compressed when you sit. Sitting on a hard surface, a long drive, or even a thick wallet in the back pocket can all flare the condition. Standing breaks every 30 minutes during the recovery window help substantially.
Will I need an MRI?
Usually no. Piriformis syndrome is a clinical diagnosis made from history and exam, and imaging is typically normal. We order an MRI when the picture is unclear, when red-flag symptoms are present, or when conservative care has not produced expected change. MRI without a clinical reason often confuses things rather than clarifying them.
Can it become chronic?
Yes if the contributing patterns continue unchanged. Going back to 10-hour days at the desk with no movement and the same wallet in the same pocket, after 6 weeks of care, is a recipe for recurrence. The maintenance side (mobility work, sitting breaks, hip strength) usually decides whether the case stays resolved.
Is there a surgery for piriformis syndrome?
A surgical release of the piriformis does exist but it is uncommon and reserved for severe cases that have failed all conservative options. Most piriformis cases resolve with the kind of layered conservative care we do, and surgery is rarely the right answer.
Insurance?
Chiropractic care may be covered. Shockwave and softwave are typically not covered by insurance. HSA/FSA accepted. Payment options →
Signs your buttock pain deserves an exam.
Piriformis is rarely an emergency, but a few patterns mean it's time to get a real plan rather than wait it out.
Deep buttock pain past 2-3 weeks
If it has not budged in two or three weeks, self-management has run its course. A structured exam differentiates piriformis from disc and shapes the plan.
Pain shooting down the leg
If the deep buttock pain is now radiating, the sciatic nerve is involved. Time-sensitive enough to evaluate, not yet an emergency.
It hurts to sit for more than 15 minutes
If your work day or your drive is being shaped by where your pain is, that is your body asking for a real fix.
Recurring after every long trip
If it comes back after every flight, road trip, or long workweek, the underlying pattern needs to change, not just the flare.
Numbness, true weakness, or foot drop
That suggests significant nerve involvement, more likely a disc than the piriformis. Either way it needs prompt evaluation.
Bowel or bladder changes · saddle numbness
Emergency room first. These are cauda equina warning signs and are not piriformis syndrome.
Let's figure out where yours actually starts.
An honest exam, an honest plan. Quickest path is a phone call.